LOS ANGELES—Sometimes the simplest interventions work best. That’s what the VA Greater Los Angeles Healthcare System discovered in its attempts to increase the number of veterans with cirrhosis who received regular surveillance for hepatocellular cancer (HCC).
Guidelines recommend that all patients with cirrhosis receive an initial screening for HCC and subsequent surveillance with abdominal ultrasound with or without serum alpha-fetoprotein (AFP) every six months. Despite system-wide efforts to improve care for VA patients with advanced liver disease, only 42% of veterans receive guideline-adherent HCC surveillance.
While other researchers explored the patient and provider barriers to surveillance, a team led by Elizabeth S. Aby, MD, of the David Geffen School of Medicine at the University of California Los Angeles, decided to try a direct approach to increasing the surveillance rate: They called all the eligible patients at the Los Angeles VA who had not had surveillance in the previous eight months.
That simple step had huge impact. Reaching a veteran by phone nearly tripled the odds that they would come in for an abdominal ultrasound, according to a study published in Hepatology Communications earlier this summer.1
The team identified 129 eligible patients who received their primary care through the VA, had specialist-confirmed diagnosed of cirrhosis, a platelet count of 150,000/uL or less, and no record of surveillance within the last eight months. Patients without contact information and those with significant comorbid conditions, including those with end-stage cancer, receiving hospice care, or with Child-Pugh C cirrhosis, for whom HCC surveillance is of limited value, were excluded.
Nearly all the eligible veterans were male (96.9%). Almost two-thirds developed cirrhosis as a complication of hepatitis C infection and 68.2% had compensated cirrhosis.
The intervention
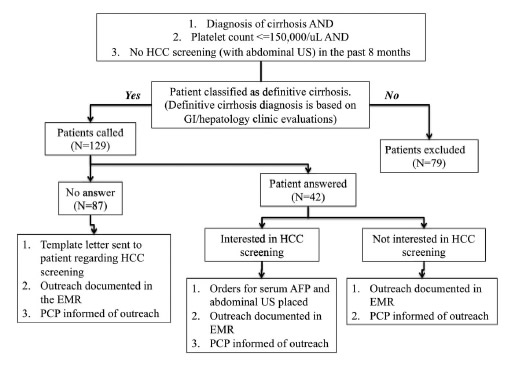
Source: Hepatology Communications, Volume: 4, Issue: 6, Pages: 825-833, First published: 24 April 2020, DOI: (10.1002/hep4.1511)
A patient navigator reached out to eligible veterans by phone to describe the risk and benefits of HCC surveillance and to assess any barriers to surveillance. The script was quick, but informative:
We are checking in to help ensure that our VA patients are receiving appropriate health screening to keep you healthy and well. As a part of our commitment to offer you the best care we are calling you to go over screening that you may be missing and arrange the best way to get them updated as soon as possible.
Has your primary care doctor ever told you that you might have problems with your liver?
If no -> Your lab results suggest that you have or may have liver disease. This means you are possibly at increased risk for developing liver cancer in the future.
Your risk of getting liver cancer increases if you have liver disease. However, screening tests can potentially find liver problems earlier so problems can be treated before they get serious.
We noticed that you are due for a liver ultrasound and a simple blood test – two screening tests for liver cancer. Research has shown that these tests can have benefits, such as fewer deaths from liver cancer.
A liver ultrasound is a quick and painless procedure. During the ultrasound, an ultrasound technologist puts some gel on your abdomen and then touches your skin with a wand to look at images of your liver on a computer screen. If the test is normal, you will be due to repeat the test in 6 months.
What questions do you have about this opportunity?
If the veteran expressed interest in proceeding with surveillance, the patient navigator scheduled the appointment for ultrasound and/or AFP testing.
If the navigator could not reach the patient by phone, they sent a letter to the veteran’s home explaining that surveillance was recommended and providing contact information to schedule the appointments.
Patient navigators connected with 32.5% of the patients by phone. The adjusted odds that the veterans contacted by phone would undergo surveillance was 2.56 times higher than those who only received letters. Almost three-quarters (72.1%) of veterans reached by phone scheduled and received abdominal imaging, while 81.8% had serum AFP completed. Surveillance identified an abdominal mass in one patient who was subsequently diagnosed with HCC.
Of the total cohort, 61.2% received abdominal imaging within six months of contact by phone or letter and 69% had serum AFP assessed during that period.
Hispanic or Latino veterans were 52% more likely than either non-Hispanic White or non-Hispanic Black veterans to receive surveillance following telephone outreach.
The team identified a negative association between hepatic encephalopathy and surveillance rates that worsened as patients had more visits with GI specialists. “More GI visits in this setting likely reflects greater illness severity, and may suggest that targeting patients with hepatic encephalopathy should be considered in future [quality improvement[ efforts,” they wrote.
Overall, the team found the result encouraging enough to continue. “Given the effectiveness of our pilot study, we will continue to invest resources in adopting intensive interventions with a multipronged approach,” Aby and her colleagues wrote. “Future interventions will make stronger efforts toward contacting patients with reminder phone calls during different hours of the day and on subsequent days in an attempt to achieve direct patient contact as well as address questions and concerns.”
As the study used volunteers for outreach, maintaining the communication effort will likely require additional resources to ensure continuity and consistency, they noted.
- Aby ES, Winters AC, Lin J, et al. A Telephone and Mail Outreach Program Successfully Increases Uptake of Hepatocellular Carcinoma Surveillance. Hepatol Commun. 2020;4(6):825-833. Published 2020 Apr 24. doi:10.1002/hep4.1511
