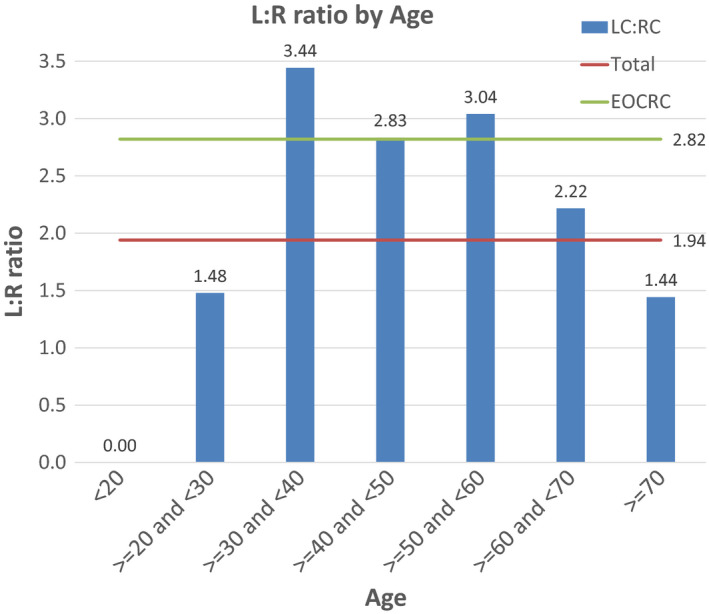
Click to Enlarge: Left to Right ratio (L:R) by age at diagnosis. The average L:R for CRC and EOCRC is represented by continuous lines Source: Cancer Medicine
ALBANY, NY — In colorectal cancer, left-sided colorectal cancer (LCC) is associated with better survival compared to right-sided colon cancer (RCC) in metastatic disease, according to a study involving VA researchers.
Past studies have indicated that older patients with Stage IV left-sided colorectal responded better to treatment and had improved overall survival. But is that true for patients younger than 50 who have early onset colorectal cancer (EOCC)?
The VA study, which involved 65,940 CRC cases from the National VA Cancer Cube Registry (2001-2015), suggested it is, but only in a limited situation. Results were published in Cancer Medicine.1
Authors from the Stratton VAMC in Albany, NY, and colleagues from the Karmanos Cancer Institute and Wayne State University, both in Detroit; Albany, NY, Medical College, and the University of Maryland in Baltimore advised that EOCRC accounts for 3.18% of cases at the VA. That’s lower than the 11% derived from the National Cancer Data Base.
“The lower fraction of EOCRC observed in our study can be accounted for by the higher incidence of malignancies in veterans than the general population,” they explained. “On average, veterans are more likely to be older, smoke, drink alcohol, and to have been exposed to Agent Orange.”
The researchers found that, “while CRC is almost twice as likely to originate from the left colon in the overall population, EOCRC is almost three times as likely to arise from the left side (L:R ratio 2.84). This ratio is highest for cases diagnosed in patients in their 30 s (L:R of 3.44).”
As for better OS survival, LCC is associated with better OS than RCC only in Stage IV for the younger patients compared to the overall population, where LCC is associated with better OS in all stages except Stage II. “The better prognosis of stage II RCC might be due to the high incidence of mismatch repair deficient tumors in this subpopulation,” the study pointed out.
“A consensus is emerging that EOCRC is a pathologically, epidemiologically, anatomically, and biologically different disease than late-onset CRC,” the researchers suggested.
The database included 2,096 EOCRC cases, defined as CRC diagnosed at younger than 50 years old. Using ICD codes, the study team defined RCC as from the cecum to the hepatic flexure (C18.0-C18.3), and LCC from the splenic flexure to the rectum (C18.5-18.7; C19 and C20).
Click to Enlarge: Left to Right ratio (L:R) by performance status. The average L:R for CRC is represented by continuous lines Source: Cancer Medicine
Results indicated that EOCRC is far more likely to originate from the left side (66.65% LCC in EOCRC vs. 58.77% in CRC). “Overall, LCC has better 5-year Overall Survival (OS) than RCC in stages I (61.67% vs. 58.01%) and III (46.1% vs. 42.1%) and better 1-year OS in stage IV (57.79% vs. 49.49%),” the researchers reported. “Stage II RCC has better 5-year OS than LCC (53.39% vs. 49.28%). In EOCRC, there is no statistically significant difference between LCC and RCC in stages I-III. Stage IV EOCRC patients with LCC and RCC have a 1-year OS of 73.23% and 59.84%, respectively.”
Background information in the article called the increase in EORCC cases “alarming,” adding, “Since 1975, there has been a 67% increase in the incidence of CRC in patients between the ages 20-49.In 2020, approximately 12% of newly diagnosed CRC cases are expected to occur in individuals under the age of 50 (17,930/147,950). Most strikingly, the fastest rise in incidence was observed in the youngest age group (20-29 years old).”
One result has been a recommendation by the American Cancer Society to lower the age of screening for people at average risk to 45.
“Screening aside, the oncology community has recognized EOCRC as an emerging unmet need,” the researchers wrote. “Specific challenges in EOCRC include a lack of understanding of the etiological drivers behind this epidemiologic increase and unfamiliarity with survivorship issues in young adults6 and a dearth of data about whether standard treatments apply to this subset.”
What Causes Early Onset?
As to what is causing the increase in early-onset colon cancer, the reasons are not clear. “Interestingly, the rise in EOCRC is driven by left-sided tumors. Additionally, a site-specific distinct molecular signature in EOCRC is emerging. Some studies suggested various potential risk factors for EOCRC as diet, stress, gut microbiota, and many others,” they added.
Touted as the first review of primary tumor sidedness (PTS) at the VA, the study noted that, while VA patients are primarily white and male, RCC is more likely to arise in women, Blacks, and the elderly. Right-sided colon cancer also tended to present at a more-advanced stage.
The article also pointed out that symptoms of CRC differ by tumor location. “Symptoms more characteristic of RCC are anemia and vague abdominal pain, while LCC usually presents with hematochezia, change in bowel habits, and is more likely to cause obstruction,” the study team noted. “This difference is thought to be due in part to the larger luminal diameter of the cecum and consistency of the bowel contents, as the tumors need to grow large enough to cause obstructive symptoms. Traditionally, this anatomical discrepancy was thought to explain the shortened survival associated with RCC. The predominance of RCC in specific epidemiologic subpopulations (Blacks, women, and elderly) belies that explanation.”
A new study from Brigham and Women’s Hospital and Harvard Medical School, also underscored the importance of colorectal cancer and how that affects tumor molecular features.
“The pathogenic effect of colorectal tumor molecular features may be influenced by several factors, including those related to microbiota, inflammation, metabolism, and epigenetics, which may change along colorectal segments,” according to the article in the Journal of Gastroenterology. “We hypothesized that the prognostic association of colon cancer location might differ by tumor molecular characteristics.”2
The international study team used a consortium dataset of 13,101 colorectal cancer cases, including 2,994 early-onset cases, to analyze how detailed tumor location stratified by statuses of microsatellite instability (MSI), CpG island methylator phenotype (CIMP), and KRAS and BRAF oncogenic mutation affected survival.
“There was a statistically significant trend for better colon cancer-specific survival in relation to tumor location from the cecum to sigmoid colon (Ptrend = 0.002), excluding the rectum,” they wrote. “The prognostic association of colon location differed by MSI status (Pinteraction = 0.001). Non-MSI-high tumors exhibited the cecum-to-sigmoid trend for better colon cancer-specific survival [Ptrend < 0.001; multivariable hazard ratio (HR) for the sigmoid colon (vs. cecum), 0.80; 95% confidence interval (CI) 0.70-0.92], whereas MSI-high tumors demonstrated a suggestive cecum-to-sigmoid trend for worse survival (Ptrend = 0.020; the corresponding HR, 2.13; 95% CI 1.15-3.92). The prognostic association of colon tumor location also differed by CIMP status (Pinteraction = 0.003) but not significantly by age, stage, or other features. Furthermore, MSI-high status was a favorable prognostic indicator in all stages.”
Those authors called for large-scale studies to examine detailed colonic subsites in molecular oncology research.
- Azar I, Al Masalmeh N, Esfandiarifard S, Virk G, Kiwan W, Frank Shields A, Mehdi S, Philip PA. The impact of primary tumor sidedness on survival in early-onset colorectal cancer by stage: A National Veterans Affairs retrospective analysis. Cancer Med. 2021 May;10(9):2987-2995. doi: 10.1002/cam4.3757. Epub 2021 Apr 2. PMID: 33797856; PMCID: PMC8085929.
- Ugai T, Akimoto N, Haruki K, Harrison TA, et. al. Prognostic role of detailed colorectal location and tumor molecular features: analyses of 13,101 colorectal cancer patients including 2994 early-onset cases. J Gastroenterol. 2023 Jan 17. doi: 10.1007/s00535-023-01955-2. Epub ahead of print. PMID: 36648535.
