Joint Trauma System Recommends Use for Trauma Resuscitation
SAN ANTONIO — For much of the history of modern medicine, whole blood was the best—and only—option for patients needing transfusion after surgery or major trauma. Beginning in the 1970s, however, the switch began from using whole blood to a component blood product, and, by 1990, whole blood was rarely used, even in battlefield situations.
While component blood reduced waste by allowing for longer storage times, it was not as effective for patients, such as wounded warriors, who needed massive transfusions. The trend to return to use of whole blood has grown, however, especially in military medicine, and received a significant boost recently with the publication of a new consensus statement from the Joint Trauma System, Defense Committee on Trauma, and Armed Services Blood Program. That group recently endorsed the use of fresh whole blood to treat hemorrhagic shock among military servicemembers.
Hemorrhage is the No. 1 cause of potentially preventable death on the battlefield, and evidence shows that early blood transfusion can reduce combat casualties. Prior to 2016, the majority of trauma resuscitation was performed using component therapy—i.e., blood that has been separated into red blood cells, plasma and platelets. Since then, the Joint Trauma System guidelines have recommended the use of whole blood.
In doing so, the military sharply diverged from civilian medicine. Fresh whole blood is not approved by the Food & Drug Administration for use in the United States because it cannot currently be as thoroughly tested for diseases. It is used in emergency combat situations in the military, however, as evidence shows it can lead to better outcomes than frozen component therapy, which requires a significant amount of time and special equipment to thaw safely.
While cold-stored whole blood also improves outcomes in trauma patients, fresh whole blood is even better for trauma resuscitation, because there is no degradation of the blood-clotting functions, said Stacy Shackelford, MD, chief of the Joint Trauma System and the lead author of the statement, which was published in the journal Transfusion.1
The major benefit of cold stored blood is that it can be thoroughly tested for infectious diseases, such as HIV and hepatitis, before transfusion. With warm fresh whole blood, the donor can be tested prior to deployment, Shackelford told U.S. Medicine. “However, there is still a delay from when they are tested to when they actually donate, so there is a small chance they could become infected with a disease.” And in rare, crisis situations in which the alternative is bleeding to death, a donor may be used who has not been tested for infections.
Easy to Transfuse

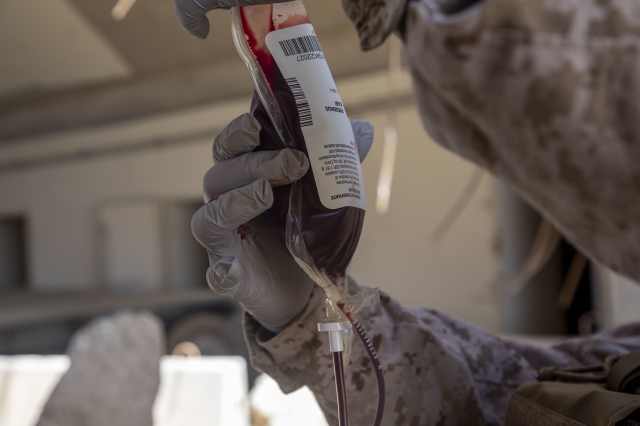
Last year, a U.S. Navy hospital corpsman, assigned to Special Purpose Marine Air-Ground Task Force – Crisis Response – Central Command 20.2, holds up a unit of blood for a simulated recipient during tactical Emergency Fresh Whole Blood Transfusion training in Kuwait. The program was is designed to place the whole blood transfusion capability into the hands of medical responders in the forward edge of the battlefield. U.S. Marine Corps photo by Sgt. Brendan Custer
Still, fresh whole blood is particularly a great choice for the military because it can be drawn from individuals on site and does not need to be shipped in from the United States, said Shackelford. “Additionally, when compared to component therapy, it is easier to transfuse in an emergency, because there is only one bag of blood to connect instead of three; it is nearly three times faster to get blood into a bleeding patient.”
This is critical, because lifesaving interventions do not improve survival if delivered too late. A 2017 study led by Shackelford analyzed records from the DoD trauma registry and found that patients who received blood product transfusion within 36 minutes of injury had a better survival rate than those who received transfusion later.2
“This was largely because the majority of deaths from bleeding occurred very early after injury,” said Shackelford. Blood transfusion should be delivered within 30 minutes after injury for severely bleeding trauma patients, according to the consensus statement. However, as Shackelford notes, “this requires a very robust trauma system plan to be able to ensure that blood transfusion is available so soon after injury.”
Although the Joint Trauma System has recommended the use of whole blood on the battlefield for five years, Shackelford said that “it has been a slow process to convert our blood program over to supply enough whole blood for trauma resuscitation.” Indeed, the statement outlines a number of logistical measures needed to support the use of whole blood. For example, it notes that deploying military personnel should undergo blood testing for transmitted disease immediately prior to deployment, and a tracking system for these prescreening results must be readily available and accessible worldwide. The authors also noted that deploying military units, particularly ground combat units, should maintain a roster of prescreened potential blood donors and should have the capability to draw fresh whole blood at or near the point of injury.
Currently, pre-deployment blood donor pre-screening is not required by the military, and Shackelford said that only a few combat units have requested it. The Armed Services Blood Program Department of Defense Instruction is currently being updated to address this gap, she said.
“Once the instruction is signed, it will still require some time to implement due to the resources needed to support; we estimate two to three years,” Shackelford explained. “There is currently a worldwide tracking system for blood products, donors and recipients; however it requires a software upgrade to support future conflict.”
Shackelford also noted that there is still a place for the use of frozen component therapy: After the initial resuscitation period, once the patient has been stabilized (about 12 to 24 hours after injury).
“If they are acutely ill from major injury, laboratory tests may show that their red cell, clotting factors, or platelets are low and require replacement,” she said. In that case, it is more efficient to measure and replace only what is needed. “These products may be used to sustain a consistently available supply of component therapy at forward locations when logistics resupply may be delayed. However, they would still need to be combined with fresh whole blood to ensure platelet blood clotting function.”
- Stacy A. Shackelford, Jennifer M. Gurney, Audra L. Taylor, Sean Keenan, et al. Joint Trauma System, Defense Committee on Trauma, and Armed Services Blood Program consensus statement on whole blood. Transfusion. Published July 16, 2021. DOI: 10.1111/trf.16454
- Stacy A. Shackelford, Deborah J. del Junco, Nicole Powell-Dunford, Edward L. Mazuchowski, et al. Association of Prehospital Blood Product Transfusion During Medical Evacuation of Combat Casualties in Afghanistan With Acute and 30-Day Survival. Journal of the American Medical Association. Published October 24, 2017. DOI: 10.1001/jama.2017.15097
