Military Researchers Find Them ‘Rare’ in Unvaccinated Adults
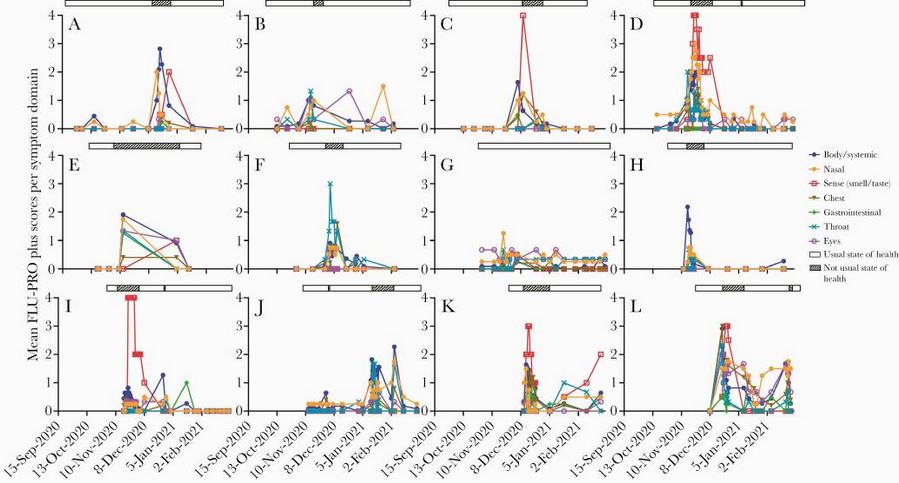
Click to Enlarge: Mean FLU-PRO Plus scores per symptom domain for SARS-CoV-2-infected participants (n = 12). FLU-PRO Plus mean scores for each of the 7 domains are represented in blue (body/systemic), orange (nasal), red (sense—smell/taste), brown (chest), green (gastrointestinal), turquoise (throat), and fuchsia (eyes); the state of health is represented by a bar above the graph (open bar: usual state of health; crosshatch bar: not usual state of health). Abbreviation: SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
BETHESDA, MD — A clear definition of the frequency of asymptomatic COVID-19 infection is important for studies estimating the prevalence of SARS-CoV-2 infection, as well as for public health measures to control the spread of this virus and its variants. Yet, estimates of the prevalence of such infections are largely inconsistent.
A recent systematic review from military researchers that incorporated large national serosurveillance studies concluded that at least one-third of SARS-CoV-2 infections are asymptomatic.
Variability in ascertaining and defining asymptomatic infections is likely due to several factors, including the patient population studied, the manner in which symptoms are assessed, the range of symptoms queried, the frequency and duration of symptom assessment and whether the study is conducted prospectively or retrospectively. Presymptomatic infection further complicates the accurate assessment of asymptomatic infection according to authors of new study, which found that asymptomatic SARS-CoV-2 infection in unvaccinated, immunocompetent adults is less common than previously reported.
In the study, researchers at the Uniformed Services University of the Health Sciences sought to determine the frequency of asymptomatic SARS-CoV-2 infections in a prospective cohort of healthcare workers. The study, published in March in Open Forum Infectious Diseases, was conducted on a subset of patients in the researchers’ Prospective Assessment of SARS-CoV-2 Seroconversion (PASS) study. The PASS study was initiated in August 2020 to prospectively evaluate the clinical and immunological responses to SARS-CoV-2 infection and vaccination in a cohort of healthcare workers at the Walter Reed National Military Medical Center (WRNMMC). The subset of participants included in the current study were those enrolled from Aug. 25, 2020, to Dec. 31, 2020.
The 263 study participants were sent a daily email reminder to complete a validated viral respiratory symptom questionnaire (FLU-PRO Plus) each day they experienced any symptoms and at least twice a month during baseline periods of health, said Emilie Goguet, PhD, research scientist at the Uniformed Services University of Health Sciences and the study’s lead author.
Asymptomatic infection was defined as no increase in total FLU-PRO Plus symptom score from each individual’s baseline values. Data included in the study were collected from Aug. 25, 2020, to Feb. 28, 2021. Throughout the study, the participants went for PCR testing whenever they had symptoms of a possible respiratory infection and had serum antibody tests on a monthly basis to capture any asymptomatic cases or cases missed by PCR testing.
Through Feb. 28, 2021, 12 participants were diagnosed with SARS-CoV-2 infection. Symptom analysis demonstrated that all 12 had at least mild symptoms of COVID-19, compared with baseline health, near or at time of infection.
“These finding suggest that completely asymptomatic infections are likely rare in unvaccinated, immunocompetent adults when symptoms are comprehensively, frequently and prospectively evaluated with standardized, validated measurement tools,” said Goguet, adding that finding was mirrored in a recent study where 90% of infected participants reported mild-to-moderate symptoms.
The study’s second key finding was that the symptoms associated with mild COVID-19 are not sufficiently distinctive to enable clinical differentiation of SARS-CoV-2 infection from other viral upper respiratory infections, Goguet said.
“While viral infectious doses and patient factors may have played a role in the clinical manifestations of SARS-CoV-2 infections in our cohort, we suspect that the high rate of symptomatic infections we observed was due to attentiveness to symptoms by study participants as well as to the prospective design of our study in which symptoms were collected throughout the fall and winter seasons, every day a person felt they had symptoms different from their baseline health,” Gouget said.
The researchers also compared symptoms that developed in the 12 participants diagnosed with COVID-19 with those of 38 participants who developed non-COVID-19 respiratory illnesses. Both groups experienced similar frequencies of runny nose, sinus pressure and sore throat. Loss of smell or taste, which were the most distinctive symptoms in patients with COVID-19, also didn’t occur with sufficient frequency or specificity to differentiate SARS-CoV-2 from non-COVID illnesses.
Goguet said it is important to highlight that the study was conducted on an unvaccinated population at the time and might not reflect rates of asymptomatic infection in vaccinated individuals. “One limitation with regards to extrapolating the findings to a different population is that our study was conducted on healthy, immunocompetent, relatively young adults—average age was 41 years old—and thus might not reflect asymptomatic rates in older populations or in individuals with comorbidities.”
These findings reinforce the need for comprehensive as well as continual monitoring of symptoms to obtain accurate measures of patient health status, she said.
The PASS study has been designed to follow the participants over a total period of four years. Not only has it provided insight into the prevalence of asymptomatic infection, but Goguet said it also has provided answers to questions such as: What are the most common symptoms associated with mild infection? Does the severity of side effects from the vaccination correlate with the strength of vaccine responses? Does the Pfizer/BioNTech mRNA vaccine offer protection against the omicron variant?
She added, “We hope that the next three years will bring more answers to the many questions we still have on the durability of the COVID-19 vaccination and, if there are baseline host factors of the innate immune system that can predict strength of immune responses to mRNA vaccination, among many others.”
- Goguet E, Powers JH 3rd, Olsen CH, Tribble DR, et. al. Prospective Assessment of Symptoms to Evaluate Asymptomatic SARS-CoV-2 Infections in a Cohort of Health Care Workers. Open Forum Infect Dis. 2022 Feb 14;9(3):ofac030. doi: 10.1093/ofid/ofac030. PMID: 35198647; PMCID: PMC8860153.
