Unexpected Results Puzzled VA Researchers
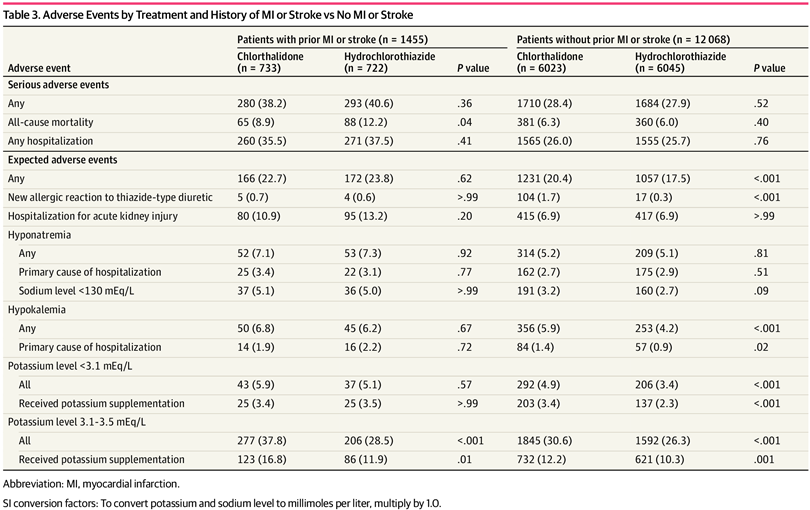
Click to Enlarge: Adverse Events by Treatment and History of MI or Stroke vs No MI or Stroke Source: JAMA Network Open
MINNEAPOLIS — Prior myocardial infarction or stroke should be taken into account when deciding to prescribe chlorthalidone (CTD) vs hydrochlorothiazide (HCTZ) in older patients with hypertension.
That is the advice from a recent study published in JAMA Network Open. The study team led by the Minneapolis VA Healthcare System asked whether, with the choice of therapy, there is a difference in major adverse cardiovascular events (MACEs) and noncancer deaths associated with and without prior myocardial infarction (MI) or stroke.
VA researchers from Boston; Memphis, TN; Washington, DC; Los Angeles and Houston, as well as associated medical schools, were also involved in the study.
The secondary analysis of a randomized clinical trial including 13,523 patients age 65 years or older found a significant qualitative interaction between the treatment group and history of MI or stroke. Specifically, participants with prior MI or stroke randomized to CTD had lower risk of MACEs and noncancer death than those receiving HCTZ.
Outcomes were not significantly different, however, in participants without prior MI or stroke.
The study team suggested its findings are important, because patients with prior MI or stroke have a greater risk of recurrent cardiovascular (CV) events. It also cautioned that the differences could have been by chance or caused by some other undiscovered factor.
The current study was a prespecified secondary analysis of the Diuretic Comparison Project (DCP), a pragmatic randomized clinical trial conducted within 72 participating VA healthcare systems from June 2016 to June 2021. Patients 65 years or older with hypertension taking HCTZ at baseline were randomized to continue HCTZ or switch to CTD at pharmacologically comparable doses. The researchers performed the secondary analysis from Jan. 3, 2023, to Feb. 29, 2024.
The focus was on the primary outcome, which consisted of a composite of stroke, MI, urgent coronary revascularization because of unstable angina, acute heart failure hospitalization or noncancer death. Additional outcomes of note included achieved blood pressure and hypokalemia (potassium level <3.1 mEq/L; to convert to mmol/L, multiply by 1.0).
The DCP randomized participants to CTD or HCTZ, with a mean (SD) study duration of 2.4 (1.4) years. At baseline for that study, median age was 72 years (IQR, 69-75 years), and 96.8% were male. Treatment effect was evaluated in subgroups of 1,455 participants with a history of MI or stroke and 12,068 without.
“There was a significant adjusted interaction between treatment group and history of MI or stroke,” the authors advised. “Participants with prior MI or stroke randomized to CTD had a lower risk of the primary outcome than those receiving HCTZ (105 of 733 [14.3%] vs. 140 of 722 [19.4%]; hazard ratio [HR], 0.73; 95% CI, 0.57-0.94; P = 0.01) compared with participants without prior MI or stroke, among whom incidence of the primary outcome was slightly higher in the CTD arm compared with the HCTZ arm (597 of 6,023 [9.9%] vs. 535 of 6,045 [8.9%]; HR, 1.12; 95% CI, 1.00-1.26; P = 0.054) (P = 0.01 for interaction).”
They added that the incidence of a nadir potassium level less than 3.1 mEq/L and hospitalization for hypokalemia differed among participants with and without prior MI or stroke when comparing those randomized to CTD vs HCTZ.
The difference was only among those:
- without prior MI or stroke (potassium level <3.1 mEq/L:
- prior MI or stroke, 43 of 733 [5.9%] vs. 37 of 722 [5.1%] [P = 0.57];
- no prior MI or stroke, 292 of 6,023 [4.9%] vs. 206 of 6045 [3.4%] [P < 0.001];
- hospitalization for hypokalemia;
- prior MI or stroke, 14 of 733 [1.9%] vs. 16 of 722 [2.2%] [P = 0.72];
- no prior MI or stroke: 84 of 6,023 [1.4%] vs 57 of 6045 [0.9%] [P = 0.02]).
“Results of this secondary analysis of the DCP trial suggest that CTD may be associated with reduced major adverse CV events and noncancer deaths in patients with prior MI or stroke compared with HCTZ,” the authors wrote.
First-Line Agents
Background information in the article noted that thiazide diuretics are recommended as first-line agents because they both lower blood pressure (BP) and prevent cardiovascular (CV) events. “There are mechanistic reasons that suggest chlorthalidone (CTD) may be superior to hydrochlorothiazide (HCTZ) for preventing CV outcomes,” the authors pointed out. “Chlorthalidone has a longer half-life and has been shown to be more effective in reducing 24-hour BP compared with HCTZ. Chlorthalidone also has other pleotropic effects, such as decreased platelet aggregation and vascular permeability mediated through inhibition of carbonic anhydrase. However, most thiazide prescriptions in the U.S. are HCTZ rather than CTD, potentially because of adverse effects associated with CTD, such as hypokalemia.”
The Diuretic Comparison Project (DCP) was a pragmatic randomized clinical trial (RCT) comparing CTD with HCTZ for the treatment of hypertension to reduce major adverse CV events (MACEs) and noncancer deaths in older U.S. veterans.
“The main trial results demonstrated no difference in effects between CTD and HCTZ on such outcomes when mostly low doses were used,” according to the subgroup analysis researchers. “However, there was a qualitative interaction between treatment group and baseline presence of MI or stroke. A qualitative interaction is when a treatment is beneficial in one subgroup but harmful in the other. The observed interaction was therefore unexpected and has not been described in prior studies, to our knowledge.”
The concerns about use of CTD remained because the “overall increase in incidence of hypokalemia in those randomized to CTD was noted irrespective of how hypokalemia was defined. The incidence of a nadir potassium level less than 3.1 mEq/L was not different between the CTD and HCTZ groups in those with prior MI or stroke. Among those without prior MI or stroke, there was a greater incidence of a nadir potassium level less than 3.1 mEq/L in the CTD group compared with the HCTZ group.”
- Ishani A, Hau C, Cushman WC, et al. Chlorthalidone vs Hydrochlorothiazide for Hypertension Treatment After Myocardial Infarction or Stroke: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw Open. 2024;7(5):e2411081. doi:10.1001/jamanetworkopen.2024.11081
