Click to Enlarge
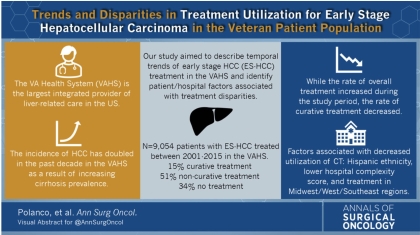
DALLAS — Veteran populations have five times the incidence of hepatocellular carcinoma (HCC)—the most common primary malignancy of the liver, which occurs largely in patients with underlying chronic liver disease—compared to the general population. The incidence of HCC has increased substantially over the last two decades within the VA Health System, primarily due to the increased prevalence of cirrhosis.
“With this elevated prevalence of HCC in the VA population, the Veterans Affairs Health System is the largest integrated provider for patients with this condition,” said Patricio Polanco, MD, associate professor of surgery in the Division of Surgical Oncology at the University of Texas Southwestern Medical Center. “Therefore,” he said, “it is relevant to know that the VA Health System as a whole is providing adequate care across all facilities nationwide.”
That, along with the increasing prevalence and incidence of hepatitis C virus (HCV)-related cirrhosis, nonalcoholic liver disease and HCC, especially within the VA population, was the motivation for a new study by Polanco and his colleagues examining HCC treatment patterns and overall survival rates across the five VAHS geographic regions.
In the retrospective study, Polanco and his colleagues used the VA Corporate Data Warehouse—containing electronic medical records from the Veterans Health Information Systems and Technology Architecture (VistA) and VHA administrative and clinical databases—to build a comprehensive national dataset of veteran patients with HCC diagnosed between 2001 and 2015 to compare patients across VAHS regions. The authors then used a multivariable Cox proportional hazards model to identify factors associated with 5-year all-cause mortality. Kaplan-Meier curves were used to visualize the patient survival function, and the log-rank test was applied to test statistical significance. In total, 13,434 patients were analyzed.
The study found treatment patterns and overall survival rates of HCC patients differ significantly across VA geographic regions.
“The West and Northeast regions had higher rates of treatments and therefore better survival,” said Polanco, who was the director of surgical oncology at the VA North Texas Health Care System/Dallas VA Medical Center at the time of the study. The Southwest had the lowest rate.
West Has Highest Treatment Rate
Specifically, the study found the West region had the highest rate of overall treatment receipt (63.6%), and the Southwest had the lowest rate (52.9%). After adjustment for demographic, clinicopathologic, treatment, and hospital factors, treatment in a non-West region continued to be significantly associated with a 10% to 13% increased risk of 5-year mortality (Midwest: hazard ratio [HR], 1.11; 95% confidence interval [CI], 1.03-1.17; Northeast: HR, 1.10; 95% CI, 1.03-1.17; Southeast: HR, 1.13; 95% CI, 1.06-1.21; Southwest: HR, 1.11; 95% CI, 1.03-1.19) (p < 0.01).
“After adjusting and controlling for patient and hospital factors, being treated at different regions for the same stage of liver cancer is associated with different chances of 5-year survival,” Polanco said. “When compared to the West regions, all the other regions had a 10-13% increased rate of mortality at 5 years for liver cancer.
“The results were not fully surprising given that even in the general population and non-VA medical systems there are significant differences in access to care, treatment and survival for different cancers across different regions,” he continued. “However, the difference in treatment receipt and mortality within the same medical system, it is still striking.”
While the data was not granular or specific enough to determine the level of care provided at each facility or the “why” of these differences in treatments, Polanco said it is safe to assume that VA facilities in larger metropolitan areas or areas where the VA hospitals are affiliated with major academic medical centers with liver cancer specialists may result in improved care and treatment outcomes.
He said targeted interventions to increase the rate of treatment in all regions are needed to improve survival of HCC veterans and provide uniformly high quality care across VA facilities, and that clinicians should be aware of differences in centers when treating patients.
“Clinicians should be aware that not all VA facilities may provide the same level of care and if these lack of liver cancer specialists—liver surgeons, oncologists, gastrointestinal liver specialists, among others, patients should be referred to a higher complexity facility as this may impact survival of patients,” Polanco said.
Risk factors for hepatocellular carcinoma have undergone dramatic changes in recent years because of more effective treatment of hepatitis. Metabolic conditions such as obesity and diabetes, as well as associated nonalcoholic fatty liver disease, now sit at the top of the list. Alcohol-use disorders also are on the increase, fueling alcoholic liver disease and alcoholic cirrhosis. At the same time, however, with more effective treatment and prevention, hepatitis C and hepatitis B infections have decreased in prevalence.
- Ju MR, Karalis JD, Chansard M, Augustine MM, Mortensen E, Wang SC, Porembka MR, Zeh HJ 3rd, Yopp AC, Polanco PM. Variation of Hepatocellular Carcinoma Treatment Patterns and Survival Across Geographic Regions in a Veteran Population. Ann Surg Oncol. 2022 Aug 26. doi: 10.1245/s10434-022-12390-7. Epub ahead of print. PMID: 36018517.
