Sickest Patients
Click to Enlarge:
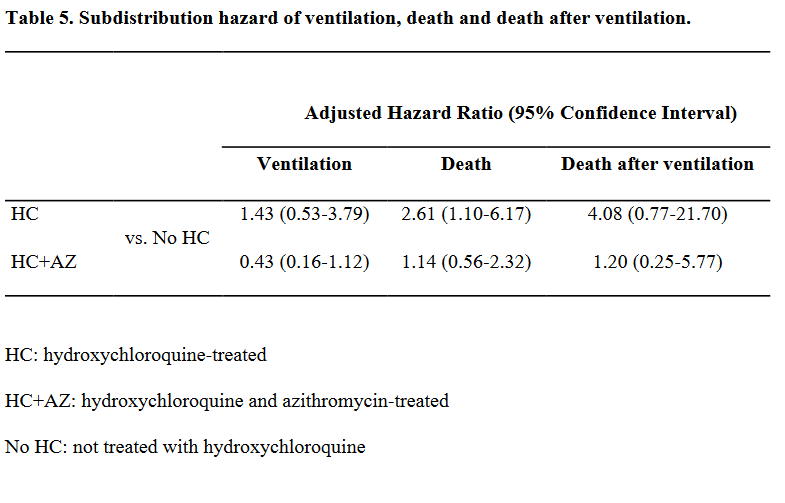
In the letter he also explained that the records used in the study looked at outcomes where hydroxychloroquine was provided to the sickest COVID-19 patients, suggesting that they were already at a higher risk for mortality.
The letter did not reassure everyone, and veterans service organizations reiterated their concerns.
“It is unknown if hydroxychloroquine is effective in treating COVID-19, and it is being given to veterans and other patients to find out,” declared Iraq and Afghanistan Veterans of America CEO Jeremy Butler. “That, by definition, makes it experimental. VA can take umbrage with our use of words, but that does not change the fact that the efficacy of using hydroxychloroquine to treat COVID-19 is unknown. In light of the results of the VA’s usage of that drug in treating patients highlighted in last week’s report, we continue to ask for clarity in the unanswered questions we raised.”
Wilkie’s assurance that VA’s use of hydroxychloroquine met medical standards was also overshadowed by evidence submitted by former HHS official Rick Bright, PhD, that there was internal strife over the drug.
Bright, who testified before Congress on May 14, alleges that he was released from his job as the leader of the Biomedical Advanced Research and Development Authority in April and moved to an NIH consulting role after resisting efforts to promote hydroxychloroquine. He describes an administration that was looking for a quick, easy treatment for the virus and sought to “flood hot spots” like New York and New Jersey with the drug.
Among the evidence submitted by Bright are email exchanges between HHS and FDA leaders that show a struggle between an administration wanting to expand the drug’s use and drug safety experts urging more caution.
The records indicate that HHS Secretary Alex Azar was pushing for an expanded access protocol which would have made the drug available outside of a hospital setting. Bright, along with Janet Woodcock, MD, director of FDA’s Center for Drug Evaluation and Research, eventually succeeded in procuring a more strict emergency use authorization, which limits the drug’s use to patients in hospitals who cannot participate in a clinical trial.
These revelations reignited concerns over hydroxychlorquine’s use at VA. In an interview with The Associated Press, Sen. Charles Schumer (D-NY) demanded answers from VA about a recent $208,000 order for more of the drug. Schumer said that Wilkie must reveal whether anyone at the White House pressured VA to include hydroxychloroquine in its treatment protocols.
Wilkie later appeared before legislators and defended VA’s use of the drug.
“Congress was very clear in saying that if people of sound mind ask to be given experimental treatments because that may be the last thing that separates them from life and death, to do that,” he declared. “There has to be hope. You can’t look at a patient and tell them you can’t have hope.”
While he said that its use had dropped in VA facilities as physicians began relying more on the antiviral remdesivir—only three patients had been treated with it the prior week—he refused to discount it entirely.
“We have to leave the door open,” Wilkie said. “With all of these studies, there still haven’t been randomized controlled trials.”
By late May, National Institute of Allergy and Infectious Diseases Director Anthony Fauci on Wednesday became the first Trump administration official to say definitively that hydroxychloroquine is not an effective treatment for the coronavirus, based on the available data.
- Magagnoli J, Narendran S, Pereira F, Cummings T, Hardin JW, Sutton SS, Ambati J. Outcomes of hydroxychloroquine usage in United States veterans hospitalized with Covid-19. medRxiv 2020.04.16.20065920; doi: https://doi.org/10.1101/2020.04.16.20065920

