BOSTON—With about 350,000 patients with heart failure diagnoses being treated in the VHA, recent studies suggesting that the cardiovascular condition increases risk of cancer have been worrisome.
Among the first of those was an article in the Journal of the American College of Cardiology, which concluded HF patients had a 68% higher risk of developing cancer (hazard ratio [HR]: 1.68; 95% CI: 1.13 to 2.50) adjusted for body mass index, smoking and comorbidities. “HF patients are at increased risk of cancer, which appears to have increased over time. Cancer increases mortality in HF, underscoring the importance of noncardiac morbidity and of cancer surveillance in the management of HF patients,” stated the Mayo Clinic researchers.1
A new study published online by the same journal has called that research into question, however. VA Boston Healthcare System researchers and colleagues suggested the trials might have been “constrained by limited size and follow-up, lack of comprehensive data on other health attributes, and adjudicated cancer outcomes.”2
The study team, which included researchers from the Hospital of the University of Pennsylvania in Philadelphia and Brigham and Women’s Hospital in Boston, among others, sought to determine to what degree HF is associated with cancer incidence and cancer-specific mortality.
Cohorts from the Physicians’ Health Studies I and II, 2 randomized controlled trials of aspirin and vitamin supplements conducted from 1982 to 1995 and from 1997 to 2011, respectively, were used to do that. Those trials included annual health evaluations and determination of cancer and HF diagnoses. The focus was on the 1,420 of the 28,341 Physicians’ Health Study participants who developed HF.
Data Analysis
The data was analyzed several ways. In the primary analysis, the study excluded participants with cancer or HF at baseline and performed multivariable-adjusted Cox models to determine the relationship between HF and cancer, modeling HF as a time-varying exposure. In a complementary analysis, the study used the landmark method and identified cancer-free participants at 70 years of age, differentiating with and without HF, performing Cox regression. In addition, sensitivity analyses were performed.
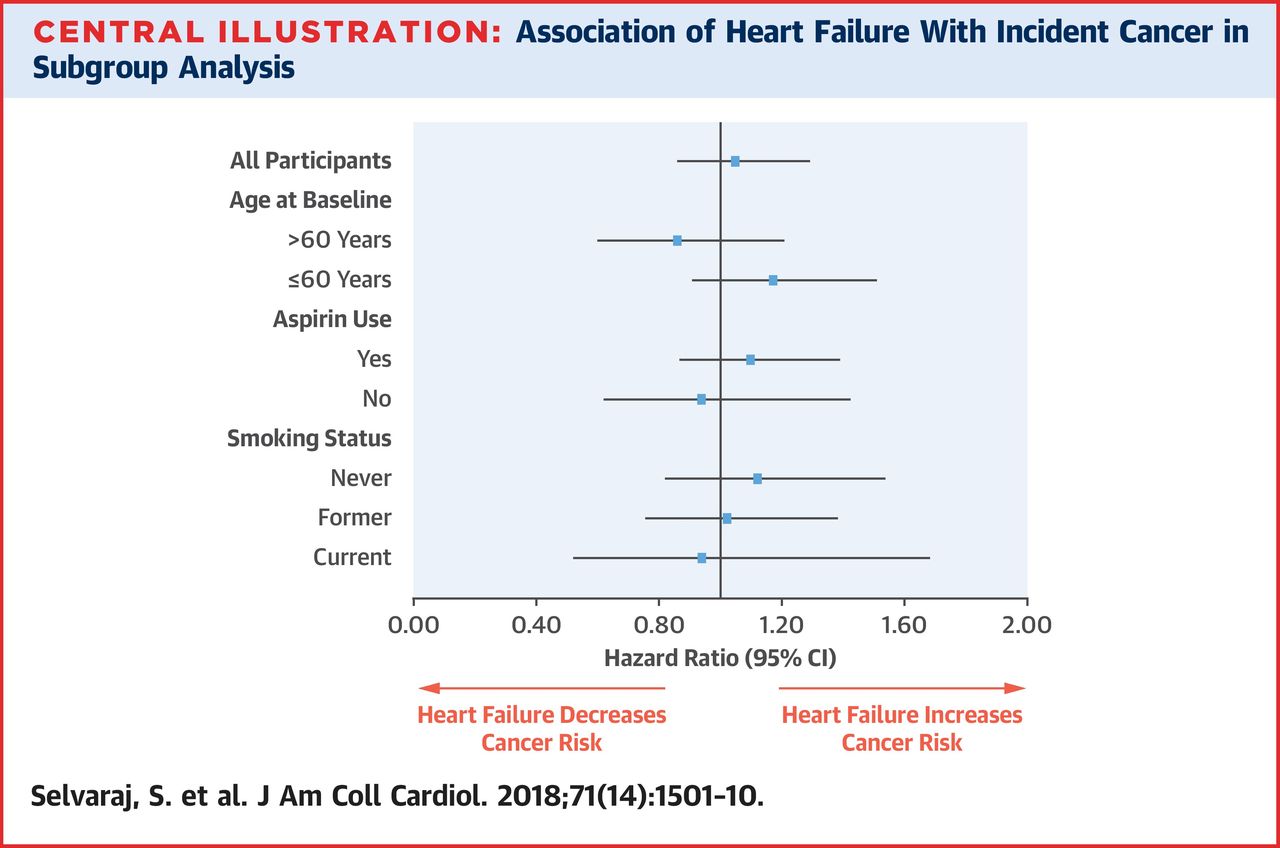
Overall, 7,363 cancers developed during a median follow-up time of 19.9 years (25th to 75th percentile: 11.0 to 26.8 years) in the group. HF was not associated with cancer incidence in crude (hazard ratio: 0.92; 95% confidence interval: 0.80 to 1.08) or multivariable-adjusted analysis (hazard ratio: 1.05; 95% confidence interval: 0.86 to 1.29), however.
In addition, the researchers reported, no association was found between HF and site-specific cancer incidence or cancer-specific mortality after multivariable adjustment. Results were similar when using the landmark method at all landmark ages, they added.
“HF is not associated with an increased risk of cancer among male physicians,” the study authors concluded.
A review in the European Journal of Heart Failure earlier this year attempted to explain the contradictory information on whether HF increases cancer risk. “This finding may be due to a surveillance bias, since active follow‐up of HF patients with regular visits may result in detection of tumors at an early stage, which is missed in the general population. Silent malignancies may be discovered by exams routinely performed for HF management (e.g., red blood cell count revealing anemia due to primary or secondary neoplastic infiltration of the bone marrow or chest X‐ray showing a pulmonary nodule).
“It is also possible that HF therapies render clinically overt tumors that would be otherwise asymptomatic: this may be for instance the case with prostate carcinoma being revealed by difficult voiding in response to diuretics, or intestinal neoplasms that start to bleed due to chronic anti‐thrombotic treatment,” the Italian authors wrote. “Strikingly, these scenarios are well known by clinical practice, but have not actually been put in evidence by the scientific literature. On the other hand, symptoms due to a tumor may overlap with those of HF and be attributed to heart disease. This may even delay cancer diagnosis, as symptoms might be thought of as due to advancing disease rather than new cancer.”
1. Hasin T, Gerber Y, McNallan SM, Weston SA, et. al. Patients with heart failure have an increased risk of incident cancer. J Am Coll Cardiol. 2013 Sep 3;62(10):881-6. doi: 10.1016/j.jacc.2013.04.088. Epub 2013 Jun 27. PubMed PMID: 23810869; PubMed Central PMCID: PMC3758775.
2. Selvaraj S, Bhatt DL, Claggett B, Djoussé L, et. Al. Lack of Association Between Heart Failure and Incident Cancer. J Am Coll Cardiol. 2018 Apr 10;71(14):1501-1510. doi:
10.1016/j.jacc.2018.01.069. PubMed PMID: 29622155.
3. Ameri P, Canepa M, Anker MS, Belenkov Y,et. al. Heart Failure Association Cardio-Oncology Study Group of the European Society of Cardiology. Cancer diagnosis in patients with heart failure: epidemiology, clinical implications and gaps in knowledge. Eur J Heart Fail. 2018 May;20(5):879-887. doi: 10.1002/ejhf.1165. Epub 2018 Feb 21. Review. PubMed PMID:29464808.
