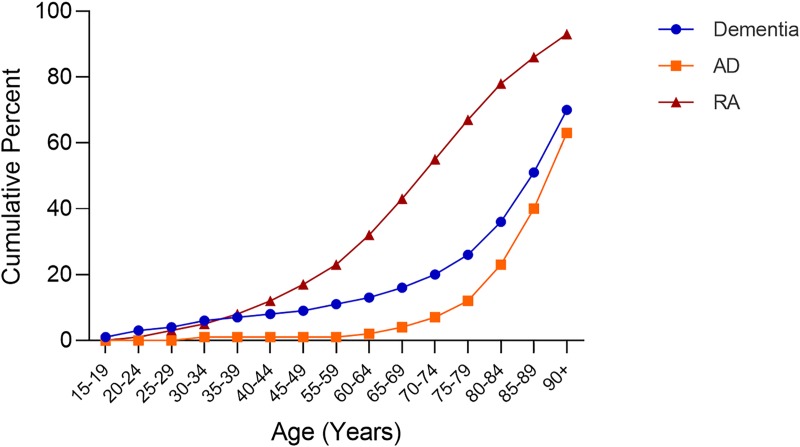
Cumulative age distribution of patients with a diagnosis code for rheumatoid arthritis, dementia or Alzheimer’s disease.
BOSTON — Alzheimer’s disease (AD) is a global health problem for which there are no disease-modifying therapies. Although the cause of Alzheimer’s and other forms of dementia is not completely understood, a growing body of evidence indicates that cerebral inflammation plays an important role and that the study of people with another inflammatory disease—rheumatoid arthritis (RA) —may provide clues into its treatment.
Because people with RA are consistently shown to have lower rates of Alzheimer’s than the general population, researchers have theorized that the therapies used to stop joint-damaging inflammation in RA may also play a role in stopping the inflammation involved in the pathogenesis of Alzheimer’s.
While studies of most conventional disease-modifying antirheumatic drugs (DMARDs) have produced mixed results in the study of Alzheimer’s, an association with tumor necrosis factor (TNF) inhibitors has been more consistent. Yet the studies have been limited, with short follow-up time, so the long-term use on of TNF use on dementia/Alzheimer’s disease remains unknown.
To better understand the long-term implications of TNF use, researchers led by Chunlei Zheng, PhD, a health scientist specialist with the VA Boston Health Care System, leveraged the long-term follow-up available for patients in the U.S. Veterans Health Administration. Using patient data from the VA Corporate Data Warehouse, a centralized database of electronic health records for patients seen at VA facilities nationwide, the researchers conducted a cohort study to investigate the association of TNF inhibitors, as a whole, or individually, with dementia risk in RA patients in the entire study period as well as different lengths of study periods—5, 10, 15 and 20 years—after RA diagnosis. The study, which involved 2,510 patients with RA prescribed TNF inhibitors, matched them 1:2 to control patients. The study period was from Jan. 1, 2000, to Aug. 24, 2020.1
Because patients with RA were often prescribed more than one TNF inhibitor in the clinical practice, the study team also compared the dementia risk between a combination of TNF inhibitors and single TNF inhibitor use in the entire study period. The researchers examined the association of TNF inhibitors with dementia in general and AD in particular. Other subtypes of dementia including vascular dementia, Lewy body and frontotemporal were not examined due to limited sample sizes.
The outcome of interest was the diagnosis of dementia during the study period.
Some key findings:
- The incidence of dementia was 5.0% and 6.0% in U.S. veterans with RA with and without TNF inhibitor treatment, respectively.
- After adjusting for age, sex, race, region, rurality, comorbidities and non-TNF drug use, patients on TNF inhibitors had significantly lower risk for dementia compared to individuals not prescribed TNF inhibitors (hazard ratio [HR]: 0 .64, CI: 0.52–0.80).
- Two commonly used TNF inhibitors, adalimumab and etanercept, were associated with an overall significantly lower risk for dementia with an HR of 0.57 (95% CI: 0.41-0.80) and 0.72 (95% CI: 0.52-0.98), respectively. (Certolizumab and golimumab were not individually analyzed, due to small sample sizes.)
- No significant difference in the dementia risk was found between patients on a combination of TNF inhibitors and those on a single agent. The researchers theorized that, because the TNF inhibitors have a similar mechanism of action, additional TNFs provided no additional benefit on reducing dementia risk.
Long-Term Risk
Similar results were seen when evaluating TNF used on long-term risk.
- TNF inhibitor use as a class were associated with lower risk for dementia in patients with RA (HRs ranging from 0.67 to 0.72 over 20 years of study period, P < 0.05).
- For individual TNF inhibitors, adalimumab showed consistent association with lower dementia risk over 20 years of study period (HRs ranging from 0.35 to 0.57, P < 0.01).
- With longer study periods and more patients developing dementia, significant association of etanercept with reduced dementia risk emerged in 20 years of study period (HR: 0.73, 95% CI: 0.54-1.00.
“We not only showed that TNF inhibitor use is associated with reduced dementia/AD risk in U.S. veterans but further provided evidence that TNF inhibitor use may have a long-term effect on decreased risk of dementia and AD in patients with RA,” the authors wrote in Alzheimer’s & Dementia. “Therefore, early reduction of neuroinflammation may have a profound impact on the pathogenesis and progression of dementia/AD.” They noted further investigation of the mechanism and potential therapeutic use of TNF inhibitors in delay of dementia/AD is warranted.
A large, retrospective case-control study of electronic health records from 56 million unique adult patients also found an effect from TNF inhibitors. Researchers from Case Western Reserve University in Cleveland and colleagues.2
The study, published in PLoS One, found that RA was associated with a higher risk for Alzheimer’s disease (Adjusted Odds Ratio (AOR) = 2.06, 95% Confidence Interval: (2.02-2.10), P-value <0.0001) as did psoriasis (AOR = 1.37 (1.31-1.42), P <0.0001), ankylosing spondylitis (AOR = 1.57 (1.39-1.77), P <0.0001), inflammatory bowel disease (AOR = 2.46 (2.33-2.59), P < 0.0001), ulcerative colitis (AOR = 1.82 (1.74-1.91), P <0.0001), and Crohn’s disease (AOR = 2.33 (2.22-2.43), P <0.0001).
“The risk for AD in patients with RA was lower among patients treated with etanercept (AOR = 0.34 (0.25-0.47), P <0.0001), adalimumab (AOR = 0.28 (0.19-0.39), P < 0.0001), or infliximab (AOR = 0.52 (0.39-0.69), P <0.0001),” the authors wrote. “Methotrexate was also associated with a lower risk for AD (AOR = 0.64 (0.61-0.68), P <0.0001), while lower risk was found in patients with a prescription history for both a TNF blocker and methotrexate. Etanercept and adalimumab also were associated with lower risk for AD in patients with psoriasis: AOR = 0.47 (0.30-0.73 and 0.41 (0.20-0.76), respectively.”
The authors pointed out that, while no effect of gender or race was identified, younger patients showed greater benefit from a TNF blocker than did older patients. “This study identifies a subset of patients in whom systemic inflammation contributes to risk for AD through a pathological mechanism involving TNF and who therefore may benefit from treatment with a TNF blocking agent,” they concluded.
- Zheng C, Fillmore NR, Ramos-Cejudo J, Brophy M, Osorio R, Gurney ME, Qui WQ, Au R, Perry G, Dubreuil M, Chen SG, Qi X, Davis PB, Do N, Xu R. Potential long-term effect of tumor necrosis factor inhibitors on dementia risk: A propensity score matched retrospective cohort study in US veterans, Alzheimer’s & Dementia. Published September 27, 2021. doi: 10.1002/alz.12465
- Zhou M, Xu R, Kaelber DC, Gurney ME. Tumor Necrosis Factor (TNF) blocking agents are associated with lower risk for Alzheimer’s disease in patients with rheumatoid arthritis and psoriasis. PLoS One. 2020 Mar 23;15(3):e0229819. doi: 10.1371/journal.pone.0229819. PMID: 32203525; PMCID: PMC7089534.
